Fallen Arches Causes And Symptoms
Overview

Fallen arches, or flatfoot, is a condition in which the arch on the inside of the foot is flat and the entire sole of the foot rests on the ground. It affects about 40 percent of the general population. Although flat feet in and of themselves are not usually problematic, they can create problems in the feet, hips, ankles and knees. Pain may be experienced in the lower legs if there are alignment problems and if the individual is engaged in a lot of heavy, high-impact activities that put stress on the bones and muscles of the lower legs.
Causes
You can have a tendency towards fallen arches from birth. Up through the toddler stage, it is common to have flat feet. Throughout childhood, arches tend to normally develop. For reasons not well understood, however, in some cases the feet stay flat and the arch never forms. In many cases this abnormality does not cause symptoms or require any treatment. In other cases, it is due to a condition called tarsal coalition. This occurs when some of the foot bones fuse.
Symptoms
Fallen arches may induce pain in the heel, the inside of the arch, the ankle, and may even extend up the body into the leg (shin splints), knee, lower back and hip. You may also experience inflammation (swelling, redness, heat and pain) along the inside of the ankle (along the posterior tibial tendon). Additionally, you may notice some changes in the way your foot looks. Your ankle may begin to turn inward (pronate), causing the bottom of your heel to tilt outward. Other secondary symptoms may also show up as the condition progresses, such as hammertoes or bunions. You may also want to check your footprint after you step out of the shower. (It helps if you pretend you?re in a mystery novel, and you?re leaving wet, footprinty clues that will help crack the case.) Normally, you can see a clear imprint of the front of your foot (the ball and the toes) the heel, and the outside edge of your foot. There should be a gap (i.e. no footprinting) along the inside where your arches are. If your foot is flat, it?ll probably leave an imprint of the full bottom of your foot-no gap to be had. Your shoes may also be affected: because the ankle tilts somewhat with this condition, the heel of your shoes may become more worn on one side than another.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
What does it mean when you have flat feet?
Non Surgical Treatment
Flexible flat feet that are painless do not require treatment. If you have pain due to flexible flat feet, an orthotic (arch-supporting insert in the shoe) can bring relief. With the increased interest in running, many shoe stores carry shoes for normal feet and pronated feet. The shoes designed for pronated feet make long distance running easier and less tiring because they correct for the abnormality. Rigid or painful flat feet require evaluation by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. If this fails to improve the pain, surgery may be necessary. For problems with the posterior tibial tendon, treatment may start with rest, anti-inflammatory medications, and shoe inserts or ankle braces. In more advanced cases, surgery may be needed to clean or repair the tendon, or fuse some of the joints of the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment

Surgical procedures for flat feet vary depending on the root cause of the condition. Surgical correction to control pronation may include bone implants or Achilles tendon lengthening. Tendon transfer, which is a procedure to re-attach a tendon to another area of bone, may also be used to reduce pronation and improve foot function.
Prevention
Flatfeet in children are often an inherited family trait, but it may be possible to prevent the condition in some cases. Recent research has shown that there are several social or cultural factors that can cause flatfeet. These factors include the following, obesity, overweight, unnecessary orthopedic treatments, wearing rigid shoes at a young age, In 1992, a study in India of 2300 children aged 4-13 demonstrated a significant difference in the rate of flatfeet among those who wore shoes regularly and those who did not. In this study, wearing inflexible, closed-toe shoes in early childhood was shown to have a negative effect on the normal development of arches. Children who were allowed to go barefoot or who wore light sandals and slippers had a much lower rate of flatfeet. In 1999, a study in Spain of 1181 children aged 4-13 revealed that the use of orthopedic shoes for treatment of flatfeet in children not only failed to correct the problem, but actually worsened the condition by preventing the normal flexing and arch development of bare or lightly protected feet. Finally, in 2006, a study of 835 children aged 3-6 showed significant differences in the rate of flatfeet based on weight, with normal-weight children having lower rates of flatfeet than children who were overweight or obese. Among adults, flatfeet due to injury, disease, or normal aging are not preventable. However, when flatfeet are related to lifestyle factors, such as physical activities, shoe selection, and weight gain, careful attention to these factors may prevent the development of flatfeet.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Fallen arches, or flatfoot, is a condition in which the arch on the inside of the foot is flat and the entire sole of the foot rests on the ground. It affects about 40 percent of the general population. Although flat feet in and of themselves are not usually problematic, they can create problems in the feet, hips, ankles and knees. Pain may be experienced in the lower legs if there are alignment problems and if the individual is engaged in a lot of heavy, high-impact activities that put stress on the bones and muscles of the lower legs.
Causes
You can have a tendency towards fallen arches from birth. Up through the toddler stage, it is common to have flat feet. Throughout childhood, arches tend to normally develop. For reasons not well understood, however, in some cases the feet stay flat and the arch never forms. In many cases this abnormality does not cause symptoms or require any treatment. In other cases, it is due to a condition called tarsal coalition. This occurs when some of the foot bones fuse.
Symptoms
Fallen arches may induce pain in the heel, the inside of the arch, the ankle, and may even extend up the body into the leg (shin splints), knee, lower back and hip. You may also experience inflammation (swelling, redness, heat and pain) along the inside of the ankle (along the posterior tibial tendon). Additionally, you may notice some changes in the way your foot looks. Your ankle may begin to turn inward (pronate), causing the bottom of your heel to tilt outward. Other secondary symptoms may also show up as the condition progresses, such as hammertoes or bunions. You may also want to check your footprint after you step out of the shower. (It helps if you pretend you?re in a mystery novel, and you?re leaving wet, footprinty clues that will help crack the case.) Normally, you can see a clear imprint of the front of your foot (the ball and the toes) the heel, and the outside edge of your foot. There should be a gap (i.e. no footprinting) along the inside where your arches are. If your foot is flat, it?ll probably leave an imprint of the full bottom of your foot-no gap to be had. Your shoes may also be affected: because the ankle tilts somewhat with this condition, the heel of your shoes may become more worn on one side than another.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
What does it mean when you have flat feet?
Non Surgical Treatment
Flexible flat feet that are painless do not require treatment. If you have pain due to flexible flat feet, an orthotic (arch-supporting insert in the shoe) can bring relief. With the increased interest in running, many shoe stores carry shoes for normal feet and pronated feet. The shoes designed for pronated feet make long distance running easier and less tiring because they correct for the abnormality. Rigid or painful flat feet require evaluation by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. If this fails to improve the pain, surgery may be necessary. For problems with the posterior tibial tendon, treatment may start with rest, anti-inflammatory medications, and shoe inserts or ankle braces. In more advanced cases, surgery may be needed to clean or repair the tendon, or fuse some of the joints of the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment
Surgical procedures for flat feet vary depending on the root cause of the condition. Surgical correction to control pronation may include bone implants or Achilles tendon lengthening. Tendon transfer, which is a procedure to re-attach a tendon to another area of bone, may also be used to reduce pronation and improve foot function.
Prevention
Flatfeet in children are often an inherited family trait, but it may be possible to prevent the condition in some cases. Recent research has shown that there are several social or cultural factors that can cause flatfeet. These factors include the following, obesity, overweight, unnecessary orthopedic treatments, wearing rigid shoes at a young age, In 1992, a study in India of 2300 children aged 4-13 demonstrated a significant difference in the rate of flatfeet among those who wore shoes regularly and those who did not. In this study, wearing inflexible, closed-toe shoes in early childhood was shown to have a negative effect on the normal development of arches. Children who were allowed to go barefoot or who wore light sandals and slippers had a much lower rate of flatfeet. In 1999, a study in Spain of 1181 children aged 4-13 revealed that the use of orthopedic shoes for treatment of flatfeet in children not only failed to correct the problem, but actually worsened the condition by preventing the normal flexing and arch development of bare or lightly protected feet. Finally, in 2006, a study of 835 children aged 3-6 showed significant differences in the rate of flatfeet based on weight, with normal-weight children having lower rates of flatfeet than children who were overweight or obese. Among adults, flatfeet due to injury, disease, or normal aging are not preventable. However, when flatfeet are related to lifestyle factors, such as physical activities, shoe selection, and weight gain, careful attention to these factors may prevent the development of flatfeet.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
True Vs. Functional Leg Length Discrepancy
Overview
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
You and your physician should discuss whether treatment is necessary. For minor LLDs in adults with no deformity, treatment may not be necessary. Because the risks may outweigh the benefits, surgical treatment to equalize leg lengths is usually not recommended if the difference is less than one inch. For these small differences, your physician may recommend a shoe lift. A lift fitted to the shoe can often improve your walking and running, as well as relieve back pain caused by LLD. Shoe lifts are inexpensive and can be removed if they are not effective. They do, however, add weight and stiffness to the shoe.

heelsncleavage
Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
You and your physician should discuss whether treatment is necessary. For minor LLDs in adults with no deformity, treatment may not be necessary. Because the risks may outweigh the benefits, surgical treatment to equalize leg lengths is usually not recommended if the difference is less than one inch. For these small differences, your physician may recommend a shoe lift. A lift fitted to the shoe can often improve your walking and running, as well as relieve back pain caused by LLD. Shoe lifts are inexpensive and can be removed if they are not effective. They do, however, add weight and stiffness to the shoe.
heelsncleavage
Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Heel Painfulness Everything You Will Need To Know Heel Aches
Overview

Plantar Fasciitis, also known as heel pain or a heel spur, is a musculoskeletal condition causing pain under the heel or into the inner arch of the foot. The condition is commonly mistaken for an impact trauma or heel bruise but in fact it is caused by mechanical overstretching of the fibrous tissue in the arch. Heel pain can develop suddenly or evolve gradually over time. It can affect people of all ages, but is more common beyond the 4th decade of life, those in standing occupations, overweight individuals and those involved in regular strenuous exercise.
Causes
Common causes of heel pain include Achilles tendinitis, Achilles tendon rupture, Bone tumor, Bursitis, Fibromyalgia, Fracture, Gout, Heel pad wear and tear, Heel spur, Osteomyelitis, Peripheral neuropathy, Pinched nerve, Plantar fasciitis, Rheumatoid arthritis, Stress fractures, Tarsal tunnel syndrome, Tendinitis. Causes shown here are commonly associated with this symptom. Work with your doctor or other health care professional for an accurate diagnosis.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
The podiatric physician will examine the area and may perform diagnostic X-rays to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, exercise and shoe recommendations, taping or strapping, or use of shoe inserts or orthotic devices. Taping or strapping supports the foot, placing stressed muscles and tendons in a physiologically restful state. Physical therapy may be used in conjunction with such treatments. A functional orthotic device may be prescribed for correcting biomechanical imbalance, controlling excessive pronation, and supporting the ligaments and tendons attaching to the heel bone. It will effectively treat the majority of heel and arch pain without the need for surgery. Only a relatively few cases of heel pain require more advanced treatments or surgery. If surgery is necessary, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation.
heel spur shoes
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
Plantar Fasciitis, also known as heel pain or a heel spur, is a musculoskeletal condition causing pain under the heel or into the inner arch of the foot. The condition is commonly mistaken for an impact trauma or heel bruise but in fact it is caused by mechanical overstretching of the fibrous tissue in the arch. Heel pain can develop suddenly or evolve gradually over time. It can affect people of all ages, but is more common beyond the 4th decade of life, those in standing occupations, overweight individuals and those involved in regular strenuous exercise.
Causes
Common causes of heel pain include Achilles tendinitis, Achilles tendon rupture, Bone tumor, Bursitis, Fibromyalgia, Fracture, Gout, Heel pad wear and tear, Heel spur, Osteomyelitis, Peripheral neuropathy, Pinched nerve, Plantar fasciitis, Rheumatoid arthritis, Stress fractures, Tarsal tunnel syndrome, Tendinitis. Causes shown here are commonly associated with this symptom. Work with your doctor or other health care professional for an accurate diagnosis.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
The podiatric physician will examine the area and may perform diagnostic X-rays to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, exercise and shoe recommendations, taping or strapping, or use of shoe inserts or orthotic devices. Taping or strapping supports the foot, placing stressed muscles and tendons in a physiologically restful state. Physical therapy may be used in conjunction with such treatments. A functional orthotic device may be prescribed for correcting biomechanical imbalance, controlling excessive pronation, and supporting the ligaments and tendons attaching to the heel bone. It will effectively treat the majority of heel and arch pain without the need for surgery. Only a relatively few cases of heel pain require more advanced treatments or surgery. If surgery is necessary, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation.
heel spur shoes
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
Mortons Neuroma Treatment
Overview
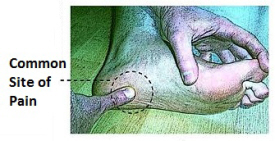
 Neuromas are generally benign or non-cancerous growths of nerve tissue, developing in various parts of the body. Morton?s Neuromas are confined to the nerves of the foot, most commonly, between the third and fourth toes. The condition involves a thickening of the tissue around one of the digital nerves leading to the toes and does not qualify as an actual tumor. The affliction causes a sharp, burning pain, usually in the region of the ball of the foot. A patient?s toes may also sting, burn or exhibit numbness. Often, the symptoms have been likened to ?walking on a marble.?
Neuromas are generally benign or non-cancerous growths of nerve tissue, developing in various parts of the body. Morton?s Neuromas are confined to the nerves of the foot, most commonly, between the third and fourth toes. The condition involves a thickening of the tissue around one of the digital nerves leading to the toes and does not qualify as an actual tumor. The affliction causes a sharp, burning pain, usually in the region of the ball of the foot. A patient?s toes may also sting, burn or exhibit numbness. Often, the symptoms have been likened to ?walking on a marble.?
Causes
The pain of Morton's neuroma occurs when the nerve connecting the toe bones (metatarsal bones) becomes irritated or compressed. The exact cause of the irritation is unknown, but it may be the metatarsal bones pressing against the nerve when the gap between the bones is narrow. This causes the nerve and surrounding tissue to thicken. Some experts believe that a number of other foot problems, including flat feet, high foot arches, bunions and hammer toes, may also play a role in Morton's neuroma.
Symptoms
Patients will feel pain that worsens with walking, particularly when walking in shoes with thin soles or high heels. Also, anything that squeezes the metatarsal heads together may aggravate symptoms, such as narrow shoes. A patient may feel the need to remove the shoe and rub the foot to soothe the pain.
Diagnosis
In some cases your doctor will be able to feel the Morton's as a swelling in the middle of your foot. However they may also suggest an X-ray or a blood test - this is normally to rule our other causes of the pain such as arthritis. The most accurate way to diagnose Morton?s itself is with magnetic resonance imaging (MRI) or ultrasound.
Non Surgical Treatment
Anti-inflammatory drugs may be recommended to dull the pain and lessen swelling. Neuropathic pain medications such as the antionvulsants and / or antidepressants may be tried as well. Many are able to recover from this issue at home by icing the area, resting the feet, and by avoiding wearing narrow or tight shoes. If these remedies do not work to alleviate symptoms, the doctor may give special devices to separate the toes and avoid the squeezing of the nerve. Steroid injections may reduce pain and swelling. Surgery may be required if these do not help.
Surgical Treatment
The ultimate success of a Morton?s neuroma treated surgically can be variable. In cases where the underlying problem is only an irritated nerve (a true Morton?s neuroma), then surgery will probably be curative (although it may take a few months for the foot to fully heal). But in many cases, forefoot pain is more complex. There may be an irritated nerve or two causing pain, but the real problem is often excessive loading of the lesser metatarsals. The generic term for this condition is metatarsalgia. When considering surgery, identifying and addressing these problems may lead to a better end result.
Prevention
While Morton?s Neuroma has been an ongoing topic of clinical investigation, the condition is in some cases difficult to either treat or prevent. Experimental efforts involving the injection of muscle or bone with chemicals such as alcohol, as well as suturing, and covering affected areas with silicone caps have been attempted, with varying success.
Neuromas are generally benign or non-cancerous growths of nerve tissue, developing in various parts of the body. Morton?s Neuromas are confined to the nerves of the foot, most commonly, between the third and fourth toes. The condition involves a thickening of the tissue around one of the digital nerves leading to the toes and does not qualify as an actual tumor. The affliction causes a sharp, burning pain, usually in the region of the ball of the foot. A patient?s toes may also sting, burn or exhibit numbness. Often, the symptoms have been likened to ?walking on a marble.?Causes
The pain of Morton's neuroma occurs when the nerve connecting the toe bones (metatarsal bones) becomes irritated or compressed. The exact cause of the irritation is unknown, but it may be the metatarsal bones pressing against the nerve when the gap between the bones is narrow. This causes the nerve and surrounding tissue to thicken. Some experts believe that a number of other foot problems, including flat feet, high foot arches, bunions and hammer toes, may also play a role in Morton's neuroma.
Symptoms
Patients will feel pain that worsens with walking, particularly when walking in shoes with thin soles or high heels. Also, anything that squeezes the metatarsal heads together may aggravate symptoms, such as narrow shoes. A patient may feel the need to remove the shoe and rub the foot to soothe the pain.
Diagnosis
In some cases your doctor will be able to feel the Morton's as a swelling in the middle of your foot. However they may also suggest an X-ray or a blood test - this is normally to rule our other causes of the pain such as arthritis. The most accurate way to diagnose Morton?s itself is with magnetic resonance imaging (MRI) or ultrasound.
Non Surgical Treatment
Anti-inflammatory drugs may be recommended to dull the pain and lessen swelling. Neuropathic pain medications such as the antionvulsants and / or antidepressants may be tried as well. Many are able to recover from this issue at home by icing the area, resting the feet, and by avoiding wearing narrow or tight shoes. If these remedies do not work to alleviate symptoms, the doctor may give special devices to separate the toes and avoid the squeezing of the nerve. Steroid injections may reduce pain and swelling. Surgery may be required if these do not help.
Surgical Treatment
The ultimate success of a Morton?s neuroma treated surgically can be variable. In cases where the underlying problem is only an irritated nerve (a true Morton?s neuroma), then surgery will probably be curative (although it may take a few months for the foot to fully heal). But in many cases, forefoot pain is more complex. There may be an irritated nerve or two causing pain, but the real problem is often excessive loading of the lesser metatarsals. The generic term for this condition is metatarsalgia. When considering surgery, identifying and addressing these problems may lead to a better end result.
Prevention
While Morton?s Neuroma has been an ongoing topic of clinical investigation, the condition is in some cases difficult to either treat or prevent. Experimental efforts involving the injection of muscle or bone with chemicals such as alcohol, as well as suturing, and covering affected areas with silicone caps have been attempted, with varying success.
Podiatrists Prefer Shoe Lifts For Leg Length Difference
There are actually two different types of leg length discrepancies, congenital and acquired. Congenital indicates that you are born with it. One leg is structurally shorter than the other. Through developmental stages of aging, the human brain senses the gait pattern and identifies some variance. The body usually adapts by tilting one shoulder over to the "short" side. A difference of less than a quarter inch isn't really excessive, demand Shoe Lifts to compensate and ordinarily won't have a serious effect over a lifetime.

Leg length inequality goes typically undiagnosed on a daily basis, yet this issue is very easily corrected, and can reduce numerous cases of back discomfort.
Treatment for leg length inequality typically involves Shoe Lifts. These are typically cost-effective, often costing less than twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most widespread health problem afflicting men and women today. Over 80 million people experience back pain at some point in their life. It is a problem which costs businesses vast amounts of money every year as a result of lost time and production. Innovative and more effective treatment solutions are always sought after in the hope of decreasing the economic influence this condition causes.

Men and women from all corners of the world suffer the pain of foot ache as a result of leg length discrepancy. In these situations Shoe Lifts are usually of worthwhile. The lifts are capable of reducing any pain in the feet. Shoe Lifts are recommended by numerous qualified orthopaedic doctors.
To be able to support the body in a well-balanced manner, the feet have got a very important role to play. Irrespective of that, it is often the most neglected area of the body. Some people have flat-feet which means there is unequal force placed on the feet. This will cause other areas of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Leg length inequality goes typically undiagnosed on a daily basis, yet this issue is very easily corrected, and can reduce numerous cases of back discomfort.
Treatment for leg length inequality typically involves Shoe Lifts. These are typically cost-effective, often costing less than twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most widespread health problem afflicting men and women today. Over 80 million people experience back pain at some point in their life. It is a problem which costs businesses vast amounts of money every year as a result of lost time and production. Innovative and more effective treatment solutions are always sought after in the hope of decreasing the economic influence this condition causes.
Men and women from all corners of the world suffer the pain of foot ache as a result of leg length discrepancy. In these situations Shoe Lifts are usually of worthwhile. The lifts are capable of reducing any pain in the feet. Shoe Lifts are recommended by numerous qualified orthopaedic doctors.
To be able to support the body in a well-balanced manner, the feet have got a very important role to play. Irrespective of that, it is often the most neglected area of the body. Some people have flat-feet which means there is unequal force placed on the feet. This will cause other areas of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Diagnosing Calcaneal Spur

Overview
A heel spur is a pointed bony outgrowth of the bone of the heel (the calcaneus bone). They are attributed to chronic local inflammation at the insertion of soft tissue tendons or fascia in the area. Heel spurs can be located at the back of the heel or under the heel, beneath the sole of the foot. Heel spurs at the back of the heel are frequently associated with inflammation of the Achilles tendon (tendinitis) and cause tenderness and pain at the back of the heel made worse while pushing off the ball of the foot.
Causes
Some causes of heel spurs include abnormal or lopsided walking, which places excessive stress on the heel bone, ligaments and nerves Running, jogging or jumping, especially on hard surfaces. Poorly fitted or badly worn shoes, especially those lacking appropriate arch support, excess weight and obesity.

Symptoms
Most bone spurs cause no signs or symptoms. You might not realize you have bone spurs until an X-ray for another condition reveals the growths. In some cases, though, bone spurs can cause pain and loss of motion in your joints.
Diagnosis
Sharp pain localized to the heel may be all a doctor needs to understand in order to diagnose the presence of heel spurs. However, you may also be sent to a radiologist for X-rays to confirm the presence of heel spurs.
Non Surgical Treatment
By reducing excessive motion and controlling and supporting the foot during physical activities an orthotic can help to limit how far the plantar fascia is pulled or torn away from the heel. A Heel Spur pad can be offered- which is a pad designed to take pressure off the spur. If the problem persists, consult your foot doctor.
Surgical Treatment
Heel spur surgery should only be considered after less invasive treatment methods have been explored and ruled insufficient. The traditional surgical approach to treating heel spurs requires a scalpel cut to the bottom of the food which allows the surgeon to access the bone spur. Endoscopic plantar fasciotomies (EPF) involve one or two small incisions in the foot which allow the surgeon to access and operate on the bone spur endoscopically. Taking a surgical approach to heel spur treatment is a topic to explore with a foot and ankle specialist.
Diagnosing Inferior Calcaneal Spur
Overview
A heel spur is a pointed bony outgrowth of the bone of the heel (the calcaneus bone). Heel spurs under the sole of the foot (plantar area) are associated with plantar fasciitis. Heel spurs and plantar fasciitis can occur alone or be related to underlying diseases. Heel spurs and plantar fasciitis are treated by measures that decrease the associated inflammation and avoid reinjury.
Causes
Though this syndrome is most common in individuals 40 years or older, it can occur at any age. The following factors increase the likelihood of heel spur development. An uneven gait which applies too much pressure to certain areas of the foot. Being overweight. Wearing worn shoes or ill-fitting footwear. Job conditions that require long periods spent standing or lifting heavy objects. The normal aging process which results in a decrease in ligament elasticity.

Symptoms
Pain and discomfort associated with heel spurs does not occur from the spur itself. The bone growth itself has no feeling. However, as you move, this growth digs into sensitive nerves and tissue along the heel of the foot, resulting in severe pain. Pain can also be generated when pushing off with the toes while walking. Swelling along the heel is also common.
Diagnosis
A thorough history and physical exam is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
Perform some exercises. Exercises that strengthen and lengthen your plantar fascia can also be very helpful for heel spurs. Try some of the following activities. Calf stretch. Place your hands on a wall. Extend 1 foot (0.3 m) behind you with your knee straight and place the other foot in front of you with the knee bent. Push your hips toward the wall and hold the stretch for 10 seconds. You should feel a pull in your calf muscles. Repeat the stretch 20 times for each foot. Plantar fascia stretch, Perform this exercise in the morning before you've done any standing or walking. Cross your injured foot over the knee of your other leg. Grasp your toes and gently pull them toward you. If you can't reach your toes, then wrap a towel around them and pull on the towel. Hold the stretch for 10 seconds and repeat 20 times for each foot.
Surgical Treatment
Surgery, which is a more radical treatment, can be a permanent correction to remove the spur itself. If your doctor believes that surgery is indicated, he will recommend an operation - but only after establishing that less drastic methods of treatment are not successful.